Health exchanges have a principal-agent problem

by Vince Hartman
Feb 06, 2026
Health exchanges have a principal-agent problem: if you market “access,” you attract buyers who value access. If you market “better care,” you attract actors willing to be accountable for outcomes.
In the US, a doctor treating you can often get immediate access to your complete medical record. That access is incredibly powerful, and leads a lot of other actors to wanting that data too. Currently, the nationwide exchange of patient data is powered by around 30 - 40 companies. I run one of them, Abstractive Health.
Doctors cannot realistically run national exchange networks themselves. That’s why these companies are entrusted with this responsibility. That’s where the principal-agent problem shows up. Doctors are the principals; health exchange companies are the agents acting on their behalf.
Broadly, these companies fall into two categories. Some market and sell products that clinicians use directly. Others market access to healthcare data itself.
Historically, electronic health records have been the dominant clinician-facing product. Epic, Oracle Health, athenahealth, and others sit in this category. Alongside them are intermediaries whose core product is data exchange or data access. These companies often sell to provider organizations, platforms, and developers, not to clinicians themselves. Abstractive Health sits in a different place. We sell directly to clinicians, but we are not an EHR. We built around a gap we believed existed in the exchange ecosystem: cognition and patient understanding, not just access to records.
This distinction matters because companies that sell directly to clinicians tend to carry less systemic risk on the exchange.
For us, our marketing is explicitly clinician-oriented. The first question we ask at signup is simply, “Are you a clinician?” Our growth is driven by whether doctors feel more prepared to care for their patients.
Provider organizations also employ product managers, engineers, and business operations teams. Those roles are often the primary buyers for data intermediaries. If you go to many exchange companies’ websites, the messaging reflects that audience. You see taglines like “universal access to health data,” “powerful data exchange,” “QHIN connectivity,” and “actionable insights.” Most clinicians don’t buy software because it says interoperability, they buy it because it helps them deliver care.
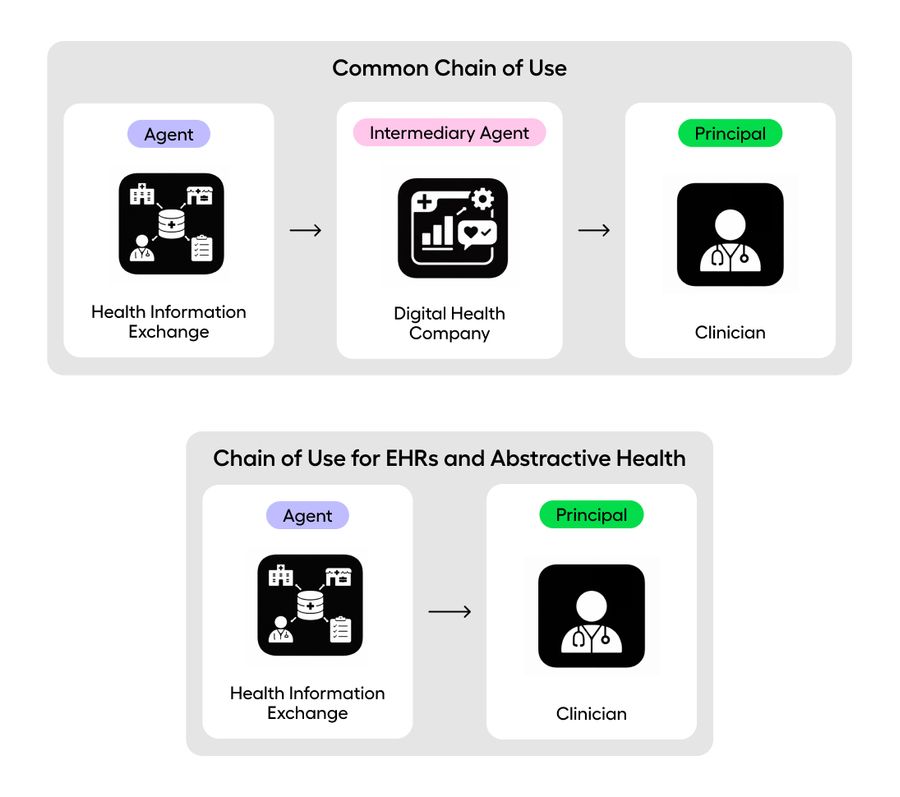
As a result, the chain of use often looks like this: an HIE company (agent) → a digital health company (intermediary agent) → a clinician (principal).
In contrast, for EHRs—and for Abstractive—the chain looks more like this: an HIE company (agent) → a clinician (principal).
There is nothing inherently wrong with selling to non-clinicians; The issue is that the risk profile is different. When users evaluate a product primarily on access to data, and not improvement in clinical experience, treatment use can drift into a compliance checkbox rather than the north star of the company.
For Abstractive, our north star is simple: AI summaries that help clinicians deliver better care. Data alone has no value to a doctor without cognition layered on top. By contrast, when a company’s north star is “improved interoperability” or “broader data access,” the culture and incentives naturally center on access itself.
A company’s customers, Ideal Customer Profile (ICP), and north star determine what it ultimately stands for. Epic’s ICP, for example, is very clear: large healthcare organizations that deliver care. Their business is oriented around that reality.
All health exchange companies carry some intrinsic risk around treatment use, but that risk sits on a spectrum. If you are a pure provider organization seeking data specifically to improve treatment, it’s rational to prefer vendors whose primary users are clinicians, and whose broader customer base cannot put your exchange access at risk. HIEs will continue to invest in governance to reduce these risks. But we are still largely avoiding the core issue: improved healthcare data access does not translate to improved treatment outcomes. The frameworks were built for treatment, but the main narrative has often been access. That narrative attracts buyers who value having the data, not necessarily using it to improve care.
The hard part here is that everyone agrees with “interoperability” in theory. Nobody wants to say no to access. But access is not the outcome, it’s the input. The outcome is whether a patient gets better care. If we keep building an ecosystem optimized around data access as the prize, it will continue to attract buyers who treat it that way.

See the Abstractive Health AI assistant in action to discover what real efficiency can look like.
Try for freeStay ahead of the curve in healthcare innovation.
Connect
Abstractive Health
Resources
©2026 Abstractive Health. All Rights Reserved.